
Diarrhea in children is one of the most common conditions parents face, especially in early childhood. Almost every child experiences at least a few episodes of acute gastroenteritis before reaching school age. In most cases, the illness is self-limiting and resolves within a few days. However, it can sometimes become serious due to the risk of dehydration. It is dehydration — not the diarrhea itself — that represents the main medical concern.
Diarrhea is defined as an increased frequency of defecation accompanied by a change in stool consistency — stools become looser, mushy, or watery. According to the World Health Organization, diarrhea is the passage of three or more loose or watery stools within a 24-hour period.
Additionally, diarrhea may be defined as stools that are more frequent than usual for the individual and of looser consistency. Stool consistency is often more clinically relevant than frequency, particularly in infants, in whom frequent bowel movements may be physiological.
Beyond frequency and consistency, so-called pathological contents in the stool are also important. In viral diarrhea, stools are typically watery, without blood and without significant amounts of mucus. The presence of mucus may suggest an inflammatory process in the colon, while visible fresh blood requires mandatory medical evaluation. Blood in the stool may result from bacterial infections caused by Shigella, Salmonella, or Campylobacter, but it may also be observed in other conditions, including anal fissures in young children. The presence of purulent material, severe foul odor, or very dark, almost black stools are also warning signs. Any change toward black discoloration or the presence of significant blood should be considered an emergency and requires immediate medical attention.
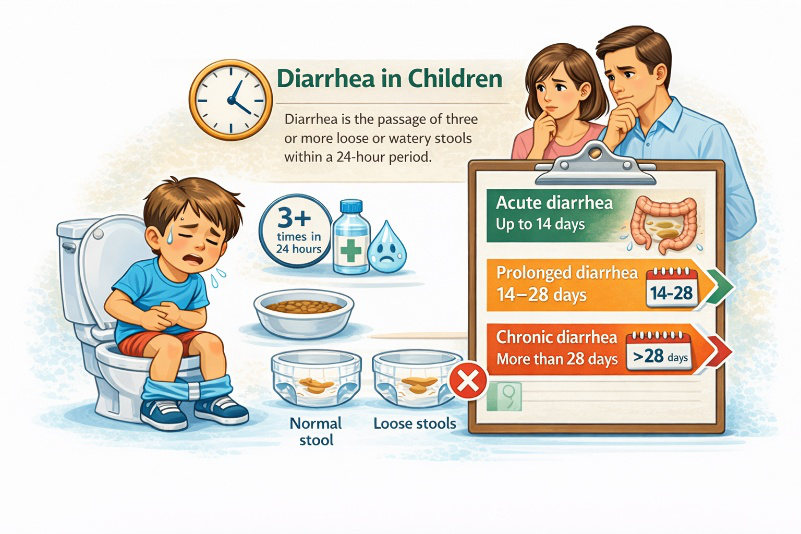
In medical practice, diarrhea is classified as acute when it lasts up to 14 days, prolonged between 14 and 28 days, and chronic when it persists for more than 28 days. In children, the acute form is the most common and is usually caused by infectious agents.
The Most Common Causes of Diarrhea in Children
The most common cause of diarrhea in childhood is viral infection. The most frequent etiological agent is Norovirus. Rotavirus also plays a leading role; in the past, it was the main cause of severe viral gastroenteritis and hospitalizations in young children. After the introduction of the rotavirus vaccine, the incidence of severe forms significantly decreased. Other common viral pathogens include adenoviruses. Viral gastroenteritis usually begins abruptly, often with vomiting, moderate fever, and watery stools. The general condition may be affected, but in most cases, symptoms resolve within a few days.

Bacterias are a less common but more severe cause of diarrhea. Among them, Salmonella, Shigella, and Campylobacter stand out. These infections more often present with high fever, abdominal pain, mucus or blood in the stool. The child may appear more toxic-appearing and may require medical evaluation and laboratory testing.
Parasitic infections are diagnosed less frequently as a cause but should be considered, especially in cases of prolonged symptoms, travel abroad, or contact with contaminated water. The most common parasitic causes in children include Giardia lamblia (Giardia intestinalis), Entamoeba histolytica, and Cryptosporidium. Parasitic gastroenteritis often presents with prolonged or intermittent diarrhea, abdominal bloating, gas, and weight loss. Fever is usually less pronounced compared to bacterial infections. In some cases, stools may be greasy and foul-smelling, especially in Giardia infection due to impaired absorption in the small intestine. Diagnosis is made through microscopic or antigen testing of stool, and treatment requires specific antiparasitic therapy.
A separate category is antibiotic-associated diarrhea, which develops after the use of antibacterial medications. It results from disruption of the normal intestinal microbiota and in some cases may be associated with infection caused by Clostridioides difficile.
Non-infectious causes should also not be forgotten — food intolerance, cow’s milk protein allergy, enzyme deficiencies, or functional disorders, which will be discussed in a separate article.
Dehydration – The Main Concern
Dehydration is a condition in which the body loses more fluids and electrolytes than it takes in. The pediatric organism is particularly vulnerable. Infants and young children have a higher percentage of total body fluids, faster metabolism, and smaller reserves. Moreover, they cannot adequately compensate for fluid losses by increasing intake, as adults can. Therefore, dehydration may develop rapidly — sometimes within 24 hours in cases of severe diarrhea and vomiting.

Clinically, dehydration is divided into mild, moderate, and severe.
Mild Dehydration (up to ~5% body weight loss)
The child may be thirsty, lips slightly dry, urine output mildly reduced, but general condition remains relatively preserved. Skin turgor is nearly normal. This is the stage in which oral rehydration is highly effective.
Moderate Dehydration (5–10%)
Dry tongue and mucous membranes, absence of tears when crying, sunken eyes, irritability or drowsiness may be observed. Pulse may be accelerated. Skin turgor is decreased — when the skin is pinched, it returns more slowly. Urination is significantly reduced. At this stage, hospital treatment is often preferred over home management.
Severe Dehydration (>10%)
This is a medical emergency. The child may appear lethargic or have altered consciousness. Cold extremities, weak or barely palpable pulse, low blood pressure, and markedly decreased or absent urine output may be present. Breathing may be rapid due to metabolic acidosis. Immediate hospital intervention, intravenous rehydration, and intensive monitoring are required.

Which Children Are at Increased Risk?
The most vulnerable are:
• Infants under 1 year of age
• Children with low body weight or malnutrition
• Children with chronic diseases
• Patients with vomiting that interferes with fluid intake
The combination of frequent diarrhea and vomiting is particularly risky, as fluid intake and retention become difficult.

How Can Parents Recognize Danger Signs?
Warning symptoms include:
• No urination for more than 6 hours in an infant
• Dry diaper
• Absence of tears
• Sunken fontanelle in babies
• Marked drowsiness
• Pale or mottled skin
In such cases, medical evaluation should not be delayed.
What Should Be Done at Home?
Treatment of acute diarrhea in children is based on three main pillars: rehydration, appropriate dietary management, and medication when necessary. The primary goal is restoration of fluid and electrolyte balance and prevention of dehydration. In most cases, proper and timely application of these measures is sufficient for a favorable outcome.
The main principle in treating acute diarrhea is rehydration. The global standard for rehydration by mouth is Oral Rehydration Therapy. It involves the intake of specially formulated solutions containing an optimal ratio of glucose and electrolytes, which help restore both fluid and electrolyte balance.

Fluids should be given in small, frequent amounts, especially if the child is vomiting. Even a few milliliters every few minutes can prevent deterioration. Breastfeeding should not be discontinued, as breast milk contains not only nutrients but also immune factors.
Plain water alone is not sufficient in cases of significant diarrhea because it does not contain necessary electrolytes. Carbonated beverages and concentrated juices may worsen the condition due to high sugar content and are not recommended.
Nutrition During Diarrhea
Modern recommendations do not support prolonged fasting. After the initial rehydration phase, light and gentle foods should be gradually introduced. Suitable options include rice, potatoes, banana, toast, boiled carrots, and light soups. Fatty and fried foods should be temporarily avoided, as well as foods high in simple sugars.

In infants, formula feeding is usually not discontinued unless there is suspicion of specific intolerance. In most cases, the gastrointestinal mucosa recovers quickly. More information about the optimal diet during diarrhea can be found here.
Medical Treatment – When Is It Necessary?
Antibiotic Therapy
Viral diarrhea does not require antibiotic treatment. Antibiotics are used only in confirmed bacterial infection or in specific clinical situations. Irrational use may prolong symptoms or lead to complications.
Probiotics – Is There Proven Effect?
Some probiotic strains have a proven moderate effect in shortening the duration of diarrhea by approximately one day. The best studied are:
• Lactobacillus rhamnosus GG
• Saccharomyces boulardii
It is important to emphasize that probiotics are an adjunct to rehydration, not a substitute.
Antiemetics
In cases of frequent vomiting that prevents oral rehydration, short-term use of an antiemetic in hospital settings may be considered. Routine home use without medical supervision is not recommended.
Antisecretory Agents
In some cases, medication that reduces intestinal secretion without suppressing motility may be used. It may shorten the duration of diarrhea in selected patients.
Antimotility Agents
Agents that suppress intestinal motility, such as loperamide, are contraindicated, especially when bacterial infection is suspected, as they may retain pathogens in the intestine and increase the risk of complications.

Antipyretics
Fever often accompanies acute gastroenteritis, especially in viral and bacterial infections. Antipyretics do not treat the cause of diarrhea but can improve the child’s general condition and reduce discomfort. The most commonly used are paracetamol and ibuprofen, administered according to body weight. They should be used rationally — when the fever causes discomfort, not solely based on a thermometer reading.
Diarrhea in Infants – Special Considerations
Diarrhea in infancy requires closer attention, as dehydration develops more rapidly and may be more severe. Infants have a higher percentage of body water and smaller physiological reserves, and their renal function is not yet fully mature, limiting their ability to concentrate urine and compensate for fluid losses. Additionally, they cannot independently express thirst or discomfort, making clinical assessment more dependent on parental observation.
Parents should carefully monitor the number of wet diapers, the infant’s tone, presence of tears when crying, and the condition of the anterior fontanelle. A sunken fontanelle, dry skin and lips, reduced feeding, and prolonged drowsiness are warning signs. The combination of diarrhea and vomiting in an infant requires particularly rapid response.

In most cases, breastfeeding should continue, as breast milk supports intestinal recovery and provides protection. With formula feeding, changing the formula is usually not necessary unless specific indications exist. The threshold for medical consultation in infants should always be lower than in older children.
When Should You Seek Medical Care?
Although most cases of acute diarrhea in children are mild and respond well to home treatment, certain situations require medical evaluation. Parents of infants under 6–12 months should be especially cautious, as dehydration develops more rapidly and may be more severe. Consultation is necessary when signs of moderate or severe dehydration are present — absence of urination for more than 6 hours in an infant or 8 hours in an older child, dry mucous membranes, absence of tears, sunken eyes or fontanelle, marked drowsiness or weakness.

Medical attention should also be sought in cases of high fever (above 38.5–39°C), especially if persistent for more than 2–3 days, as well as when blood or significant mucus is present in the stool. Severe localized abdominal pain, repeated uncontrollable vomiting that prevents fluid intake, or worsening general condition are also warning signs. In children with chronic diseases, immune deficiency, or malnutrition, the threshold for consultation should be lower.
If a parent feels that the child “does not look as usual” or the condition worsens despite measures taken, it is better to seek timely evaluation than to miss the onset of complications.
Diagnosis and Differential Diagnosis
Diagnosis of acute diarrhea in children is primarily clinical, based on medical history and physical examination. It is important to assess stool frequency and consistency, duration of symptoms, presence of vomiting, fever, pathological stool contents, and signs of dehydration. Laboratory tests are not necessary in mild cases but are recommended in severe conditions, persistent high fever, blood in the stool, or suspicion of bacterial infection.
Differential diagnosis includes food intolerance (e.g., secondary lactose intolerance), cow’s milk protein allergy, intussusception, appendicitis, urinary tract infection in infants, and chronic inflammatory or malabsorption conditions in cases of prolonged diarrhea.
Prevention of Diarrhea in Children
Prevention of acute gastroenteritis in childhood is based on good hygiene, safe food handling, and specific immunization. The most effective measure against severe viral forms is rotavirus vaccination, which significantly reduces the risk of hospitalization and complications in infancy. Vaccination does not prevent all cases of rotavirus diarrhea but reduces severe forms and dehydration.
Regular and proper handwashing remains a key preventive measure, especially after diaper changes, using the toilet, and before meals. Viruses such as Norovirus are highly contagious and can spread rapidly in childcare settings, therefore isolation of the sick child until symptoms resolve is recommended. Surfaces at home should be cleaned regularly, especially in cases of vomiting.

Safe food storage and proper thermal preparation are essential to prevent bacterial infections such as Salmonella and Campylobacter. When traveling to areas with lower sanitation standards, consumption of untreated water and raw foods should be avoided.
Breastfeeding has a protective effect due to antibodies and immune factors present in breast milk. Maintaining good nutritional status also reduces the risk of severe disease in case of infection.
Conclusion
Diarrhea in children is a common and potentially serious condition. In most cases, it resolves without complications when timely and proper rehydration is applied. The most important task for parents is to recognize signs of dehydration and not underestimate deterioration in general condition. When in doubt, it is always better to seek medical evaluation.

Important Notice
The information in this article is educational and informational in nature. It does not replace a medical examination, diagnosis, or individual consultation with a physician. In cases of persistent symptoms, signs of dehydration, high fever, blood in the stool, or worsening general condition, timely medical evaluation is required.
About the Author
Dr. Angel Todev is a specialist in infectious diseases with clinical experience in the diagnosis and treatment of acute and chronic infectious diseases in children and adults.